True or False ...
Brain imaging may be clinically useful in psychiatry, such as in determining appropriate treatments for patients
Read on to find out!
Brain imaging may be clinically useful in psychiatry, such as in determining appropriate treatments for patients
Read on to find out!
TRUE!
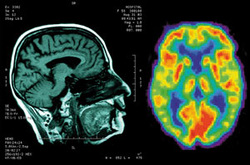
Brain imaging is being incorporated more and more into psychiatry related research, particularly in investigations of mental illnesses. Furthermore, certain studies have demonstrated optimistic results and suggest that brain imaging could hold clinical utility for the field in helping not only to diagnose patients, but more especially to determine the treatments that are right for them.
One such study is by Dr. Helen Mayberg and colleagues, who suggest PET scans may be beneficial in determining among patients diagnosed with major depression, which intervention they will better respond to: antidepressant treatment or Cognitive Beharioural Therapy.
Brain imaging is being incorporated more and more into psychiatry related research, particularly in investigations of mental illnesses. Furthermore, certain studies have demonstrated optimistic results and suggest that brain imaging could hold clinical utility for the field in helping not only to diagnose patients, but more especially to determine the treatments that are right for them.
One such study is by Dr. Helen Mayberg and colleagues, who suggest PET scans may be beneficial in determining among patients diagnosed with major depression, which intervention they will better respond to: antidepressant treatment or Cognitive Beharioural Therapy.
For more on Dr. Mayberg and colleagues' study, the abstract of their journal article can be found below, in addition to links to other news articles that have referenced this interesting finding.
Toward a neuroimaging treatment selection biomarker for major depressive disorder.
McGrath CL, Kelley MD, Holzheimer III PE, Dunlop BW, Craighead WE, Franco AR, Craddock RC, Mayberg HS.
June 12, 2013, JAMA Psychiatry
Importance Currently, fewer than 40% of patients treated for major depressive disorder achieve remission with initial treatment. Identification of a biological marker that might improve these odds could have significant health and economic impact.
Objective To identify a candidate neuroimaging “treatment-specific biomarker” that predicts differential outcome to either medication or psychotherapy.
Design Brain glucose metabolism was measured with positron emission tomography prior to treatment randomization to either escitalopram oxalate or cognitive behavior therapy for 12 weeks. Patients who did not remit on completion of their phase 1 treatment were offered enrollment in phase 2 comprising an additional 12 weeks of treatment with combination escitalopram and cognitive behavior therapy.
Setting Mood and anxiety disorders research program at an academic medical center.
Participants Men and women aged 18 to 60 years with currently untreated major depressive disorder.
Intervention Randomized assignment to 12 weeks of treatment with either escitalopram oxalate (10-20 mg/d) or 16 sessions of manual-based cognitive behavior therapy.
Main Outcome and Measure Remission, defined as a 17-item Hamilton Depression Rating Scale score of 7 or less at both weeks 10 and 12, as assessed by raters blinded to treatment.
Results Positive and negative predictors of remission were identified with a 2-way analysis of variance treatment (escitalopram or cognitive behavior therapy) × outcome (remission or nonresponse) interaction. Of 65 protocol completers, 38 patients with clear outcomes and usable positron emission tomography scans were included in the primary analysis: 12 remitters to cognitive behavior therapy, 11 remitters to escitalopram, 9 nonresponders to cognitive behavior therapy, and 6 nonresponders to escitalopram. Six limbic and cortical regions were identified, with the right anterior insula showing the most robust discriminant properties across groups (effect size = 1.43). Insula hypometabolism (relative to whole-brain mean) was associated with remission to cognitive behavior therapy and poor response to escitalopram, while insula hypermetabolism was associated with remission to escitalopram and poor response to cognitive behavior therapy.
Conclusions and Relevance If verified with prospective testing, the insula metabolism-based treatment-specific biomarker defined in this study provides the first objective marker, to our knowledge, to guide initial treatment selection for depression.
Links to other news articles that have referenced this study:
Toward a neuroimaging treatment selection biomarker for major depressive disorder.
McGrath CL, Kelley MD, Holzheimer III PE, Dunlop BW, Craighead WE, Franco AR, Craddock RC, Mayberg HS.
June 12, 2013, JAMA Psychiatry
Importance Currently, fewer than 40% of patients treated for major depressive disorder achieve remission with initial treatment. Identification of a biological marker that might improve these odds could have significant health and economic impact.
Objective To identify a candidate neuroimaging “treatment-specific biomarker” that predicts differential outcome to either medication or psychotherapy.
Design Brain glucose metabolism was measured with positron emission tomography prior to treatment randomization to either escitalopram oxalate or cognitive behavior therapy for 12 weeks. Patients who did not remit on completion of their phase 1 treatment were offered enrollment in phase 2 comprising an additional 12 weeks of treatment with combination escitalopram and cognitive behavior therapy.
Setting Mood and anxiety disorders research program at an academic medical center.
Participants Men and women aged 18 to 60 years with currently untreated major depressive disorder.
Intervention Randomized assignment to 12 weeks of treatment with either escitalopram oxalate (10-20 mg/d) or 16 sessions of manual-based cognitive behavior therapy.
Main Outcome and Measure Remission, defined as a 17-item Hamilton Depression Rating Scale score of 7 or less at both weeks 10 and 12, as assessed by raters blinded to treatment.
Results Positive and negative predictors of remission were identified with a 2-way analysis of variance treatment (escitalopram or cognitive behavior therapy) × outcome (remission or nonresponse) interaction. Of 65 protocol completers, 38 patients with clear outcomes and usable positron emission tomography scans were included in the primary analysis: 12 remitters to cognitive behavior therapy, 11 remitters to escitalopram, 9 nonresponders to cognitive behavior therapy, and 6 nonresponders to escitalopram. Six limbic and cortical regions were identified, with the right anterior insula showing the most robust discriminant properties across groups (effect size = 1.43). Insula hypometabolism (relative to whole-brain mean) was associated with remission to cognitive behavior therapy and poor response to escitalopram, while insula hypermetabolism was associated with remission to escitalopram and poor response to cognitive behavior therapy.
Conclusions and Relevance If verified with prospective testing, the insula metabolism-based treatment-specific biomarker defined in this study provides the first objective marker, to our knowledge, to guide initial treatment selection for depression.
Links to other news articles that have referenced this study:
- Scan Predicts Whether Therapy or Meds Will Best Lift Depression (National Institute of Mental Health)
- New Uses of Brain Imaging Get Closer to Clinic (Psychiatric News from the APA)
 RSS Feed
RSS Feed
