Agitation in the emergency department is not unusual. In fact, agitation can be due to a variety of psychiatric disorders including schizophrenia, bipolar disorder, major depression, anxiety and personality disorders, in addition to also being associated with medical and neurologic ailments including delirium, "brain" diseases, substance use, and medications. Medical professionals and the involvement of police or other authorities can also contribute to the development of agitation for some patients.
Up until recently, most guidelines on agitation were heavily focused on the use of medications for behaviour control. In a survey of Psychiatric Emergency Service directors, many also admitted that they used the same medication regime (often a combination of Ativan and Haldol) regardless of the patient's diagnosis, and despite there being other nonpharmacologic options to address agitation.
As a result of this, the American Association for Emergency Psychiatry developed Project BETA in 2010. The idea behind this project was through disseminating evidence and consulting experts in the field, new guidelines could be developed for the management of agitation in the ED setting that were not only effective in treating agitation, but were also patient-centered and safe.
While the complete guidelines are available below, the main gist of Project BETA is that the preferred method for managing the agitated patient should be to use verbal de-escalation. It is also recommended that de-escalation should take precedence over use of emergency medications, seclusion, or restraints, unless signs or symptoms warrant more urgent intervention.
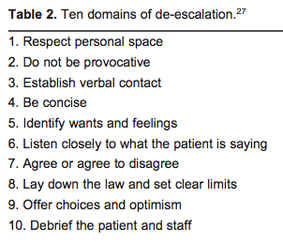
As was further discussed at the 2014 PsychSIGN conference by Dr. Rachel Lipson Glick, a internist turned psychiatrist, who is now the medical director of the Psychiatric Emergency Service at the University of Michigan, In specific regards to verbal de-escalation, there are 10 components that can be utilized to help calm a patient. In some situations medication may truly be beneficial to a patient, and so providing the patient with options, such as receiving medication, and including them in the decisions is included as a feature of the de-escalation process.
You can read more about verbal de-escalation and Project BETA below. Definitely worth a read if you are going to be working in an ED at any time during your clerkship or residency!
Up until recently, most guidelines on agitation were heavily focused on the use of medications for behaviour control. In a survey of Psychiatric Emergency Service directors, many also admitted that they used the same medication regime (often a combination of Ativan and Haldol) regardless of the patient's diagnosis, and despite there being other nonpharmacologic options to address agitation.
As a result of this, the American Association for Emergency Psychiatry developed Project BETA in 2010. The idea behind this project was through disseminating evidence and consulting experts in the field, new guidelines could be developed for the management of agitation in the ED setting that were not only effective in treating agitation, but were also patient-centered and safe.
While the complete guidelines are available below, the main gist of Project BETA is that the preferred method for managing the agitated patient should be to use verbal de-escalation. It is also recommended that de-escalation should take precedence over use of emergency medications, seclusion, or restraints, unless signs or symptoms warrant more urgent intervention.
As was further discussed at the 2014 PsychSIGN conference by Dr. Rachel Lipson Glick, a internist turned psychiatrist, who is now the medical director of the Psychiatric Emergency Service at the University of Michigan, In specific regards to verbal de-escalation, there are 10 components that can be utilized to help calm a patient. In some situations medication may truly be beneficial to a patient, and so providing the patient with options, such as receiving medication, and including them in the decisions is included as a feature of the de-escalation process.
You can read more about verbal de-escalation and Project BETA below. Definitely worth a read if you are going to be working in an ED at any time during your clerkship or residency!
 RSS Feed
RSS Feed
